Optimization of SPECT/CT based lung dose calculation for Holmium-166 hepatic radioembolization
- 1. Department of Radiology and Nuclear Medicine, University Medical Center Utrecht
Description
Background: Quantitative SPECT of the lungs after intra-arterial hepatic radioembolization using Holmium-166 (166Ho)microspheres is essential to assess therapy safety. A SPECT estimated lung absorbed dose resulting from radioembolization of more than 30 Gy is a contra-indication for therapy. Earlier we showed the superiority of Monte Carlo-based iterative reconstructions over conventional reconstructions due to its quantitative nature, required for dosimetry, at the cost of substantial computation times. In clinical routine, however, the limited available time between scout imaging and therapy constrains its application. To reduce computation times, we investigated the minimum number of iterations required to guarantee a clinical acceptable accuracy in lung dose estimation using patient and phantom data.
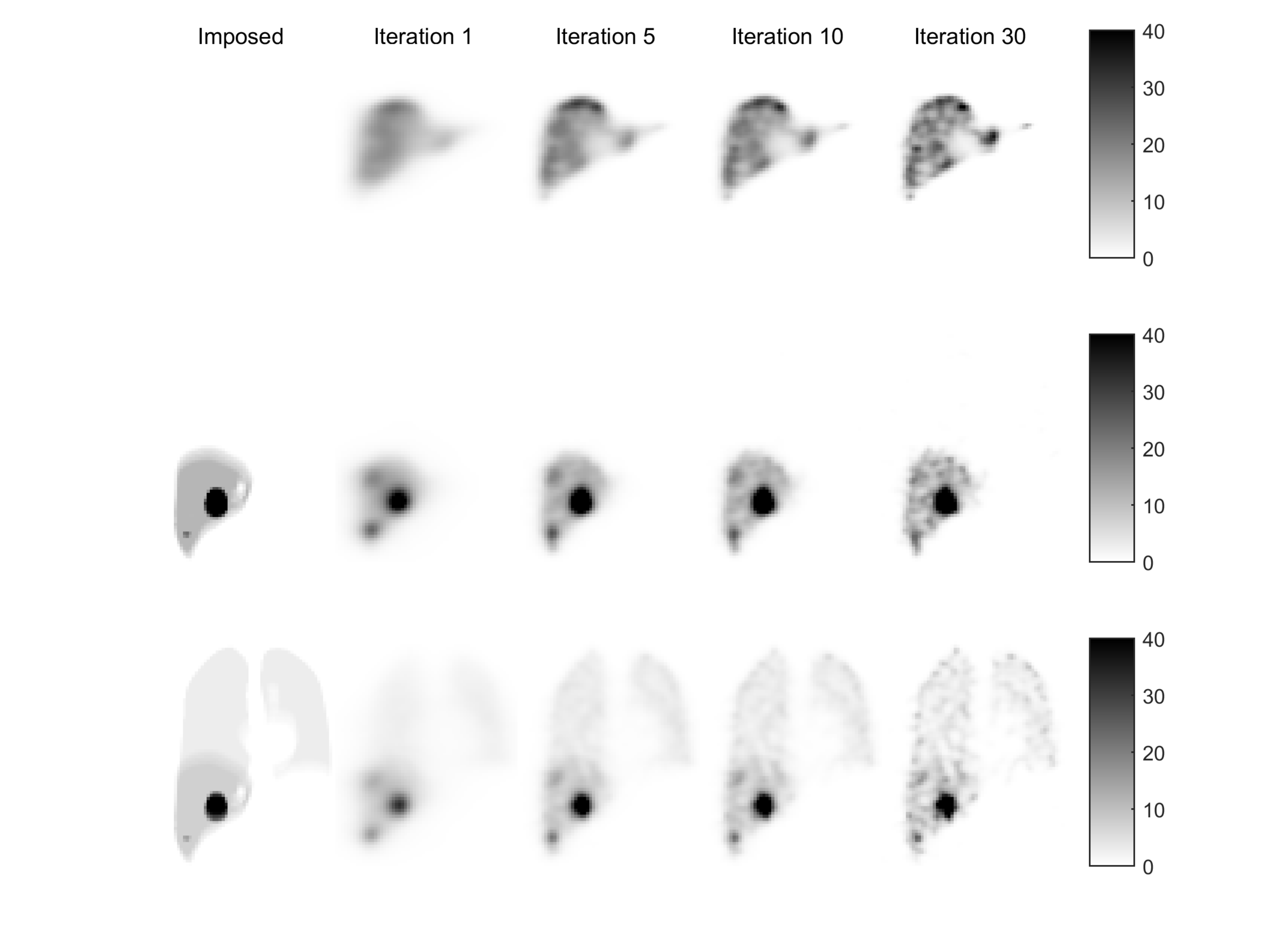
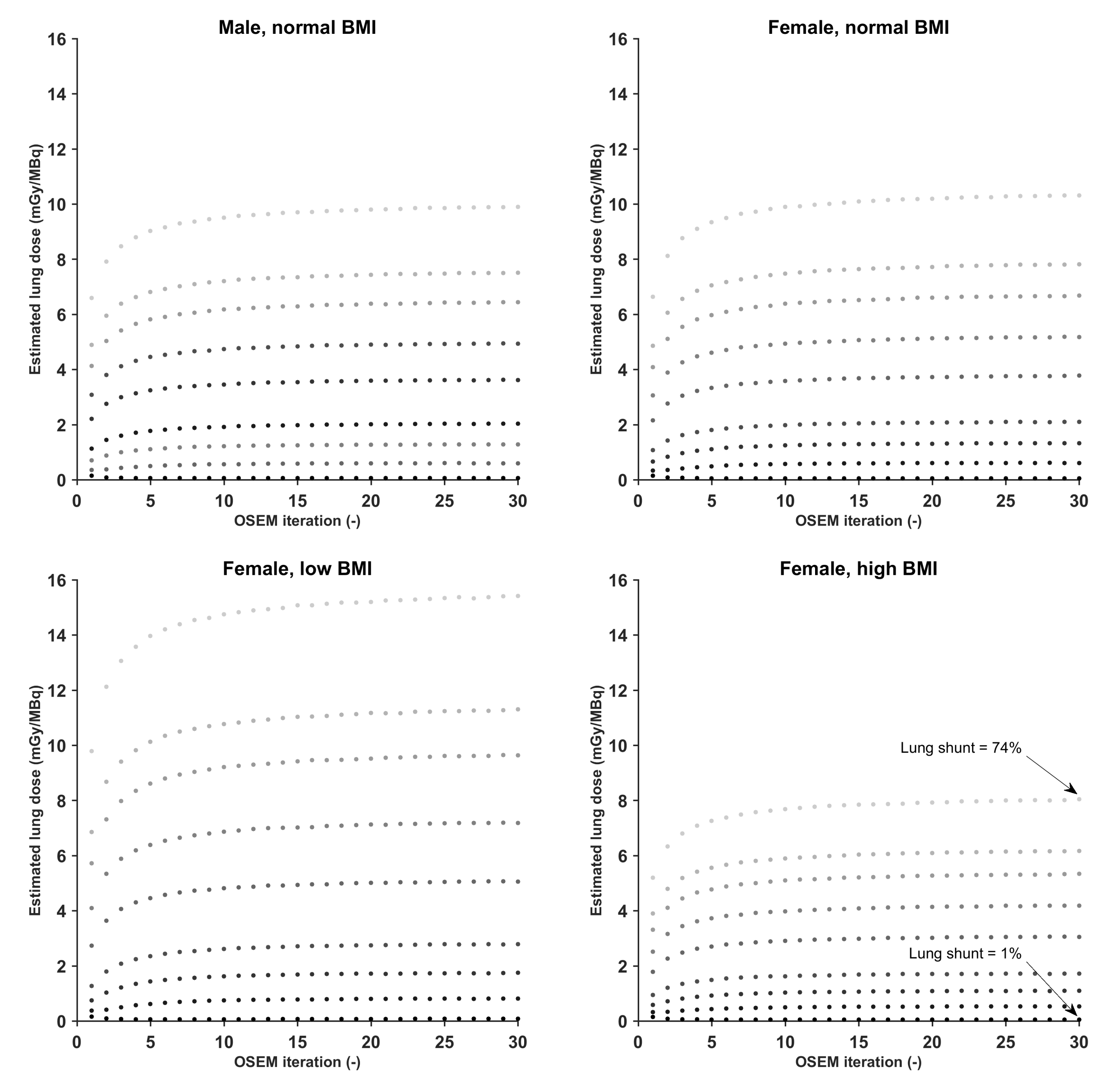
Methods: 166Ho scout SPECT data (range: 222-283 MBq) were used from 9 patients. SPECT images were Monte Carlo-based OSEM reconstructed (iterations: 30, subsets: 8). Additionally, the 4D XCAT anthropomorphic phantom was used to mimic SPECT studies with an injected scout activity of 250 MBq and with varying lung doses ranging from 0 to 15.6 mGy/MBq. These studies were reconstructed in the same way as the patient data.
Results: In all patients the lung absorbed dose upon OSEM convergence ranged from 0 to 0.025 mGy/MBq, and ranged from 0.002 to 0.078 mGy/MBq after five iterations, still well below the allowed 30 Gy in case treatment was proceeded. In the phantom data, the estimated lung dose ranged from 0.004 to 15 mGy/MBq upon convergence and from 0.03 to 13.9 mGy/MBq after five iterations, simulating situations well below and above an estimated treatment lung dose of 30 Gy. Importantly, the lung absorbed dose upon OSEM convergence was underestimated by 15% as compared to the actual simulated lung dose, and the dose after five OSEM iterations was underestimated by 9% as compared to the dose upon convergence. Both underestimations were irrespective of the magnitude of the lung dose and thus can be easily corrected for.
Conclusions: The number of OSEM iterations necessary for a quantitative estimate of the lung dose can be reduced from 30 to 5. The resulting six fold reduction in calculation time enables data processing of the scout images before therapy administration.
Files
Figure1.png
Files
(163.3 MB)
| Name | Size | Download all |
|---|---|---|
|
md5:330d90213cd054bb69fc9c4c5f384dbd
|
12.2 MB | Download |
|
md5:4edbd98255d46233ecb1c4b7a0c52d64
|
437.0 kB | Preview Download |
|
md5:534112773dc877e6e5e8eb1e30226c22
|
149.4 MB | Download |
|
md5:7bb568c71a05b5b60e7cbfeb677733b5
|
244.4 kB | Preview Download |
|
md5:bd7fc70c65833bb1bd4ba6c1fd69941c
|
3.5 kB | Download |
|
md5:19561f2d6f8dbab265a0b44641e18125
|
205.4 kB | Preview Download |
|
md5:6c264771b8af27f09a7752bb7e6e4d09
|
8.9 kB | Download |
|
md5:19c4726e47d104c3b8609fc30522c6f5
|
489.2 kB | Preview Download |
|
md5:8aad5cd6803b0a567ce6bd12789f2535
|
934 Bytes | Download |
|
md5:2f0b02869bd8776f7f2a12240cf381a7
|
139.5 kB | Preview Download |
|
md5:5cb891a93c561b0d41087b470f4a0029
|
906 Bytes | Download |
|
md5:13eeef4f79ae664438a24ad143351231
|
116.7 kB | Preview Download |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}